
Iron deficiency anemia affects up to 50% of pregnant women worldwide, creating a critical challenge for both maternal and fetal health. As your blood volume expands dramatically during pregnancy, your iron requirements surge to support your growing baby’s development and your own physiological changes. When dietary sources and oral supplements fail to meet these increased demands—whether due to intolerance, malabsorption, or late diagnosis—intravenous iron infusion becomes a vital therapeutic option. Understanding the precise clinical guidelines for iron infusion in pregnancy ensures you receive timely, effective treatment without unnecessary delays that could compromise your health or your baby’s development.
This comprehensive guide details the exact criteria, protocols, and safety considerations that determine when iron infusion becomes necessary during pregnancy. You’ll discover how healthcare providers assess your specific situation, which modern IV iron formulations offer the safest profile, and what to realistically expect during and after treatment—all based on current medical evidence and clinical best practices.
Why Iron Stores Deplete Rapidly During Pregnancy
Your iron needs multiply significantly from the moment you conceive, creating a perfect storm for deficiency that many women struggle to overcome through diet alone. The placenta requires approximately 250-300mg of iron for proper development, while your expanding blood volume demands another 500mg to support increased red blood cell production. Your baby then draws heavily from your reserves during the third trimester, accumulating 250-350mg of iron to sustain those crucial first months after birth.
This dramatic increase transforms your daily iron requirement from 18mg for non-pregnant women to 27mg or more—a 50% jump that proves difficult to achieve through food sources alone. While your body becomes more efficient at absorbing iron during pregnancy (up to three times more than normal), this adaptation often falls short, particularly if your pre-pregnancy iron stores were already marginal. Vegetarian and vegan mothers face even greater challenges, as plant-based iron (non-heme) absorbs at only half the rate of animal-based (heme) iron.
The progression from depleted iron stores to full-blown anemia typically follows three stages:
- Stage 1: Declining ferritin levels (below 30 ng/mL) with normal hemoglobin
- Stage 2: Reduced iron transport capacity with borderline hemoglobin
- Stage 3: Frank iron deficiency anemia with hemoglobin below trimester-specific thresholds
Recognizing these stages early allows for timely intervention before your baby’s development becomes compromised.
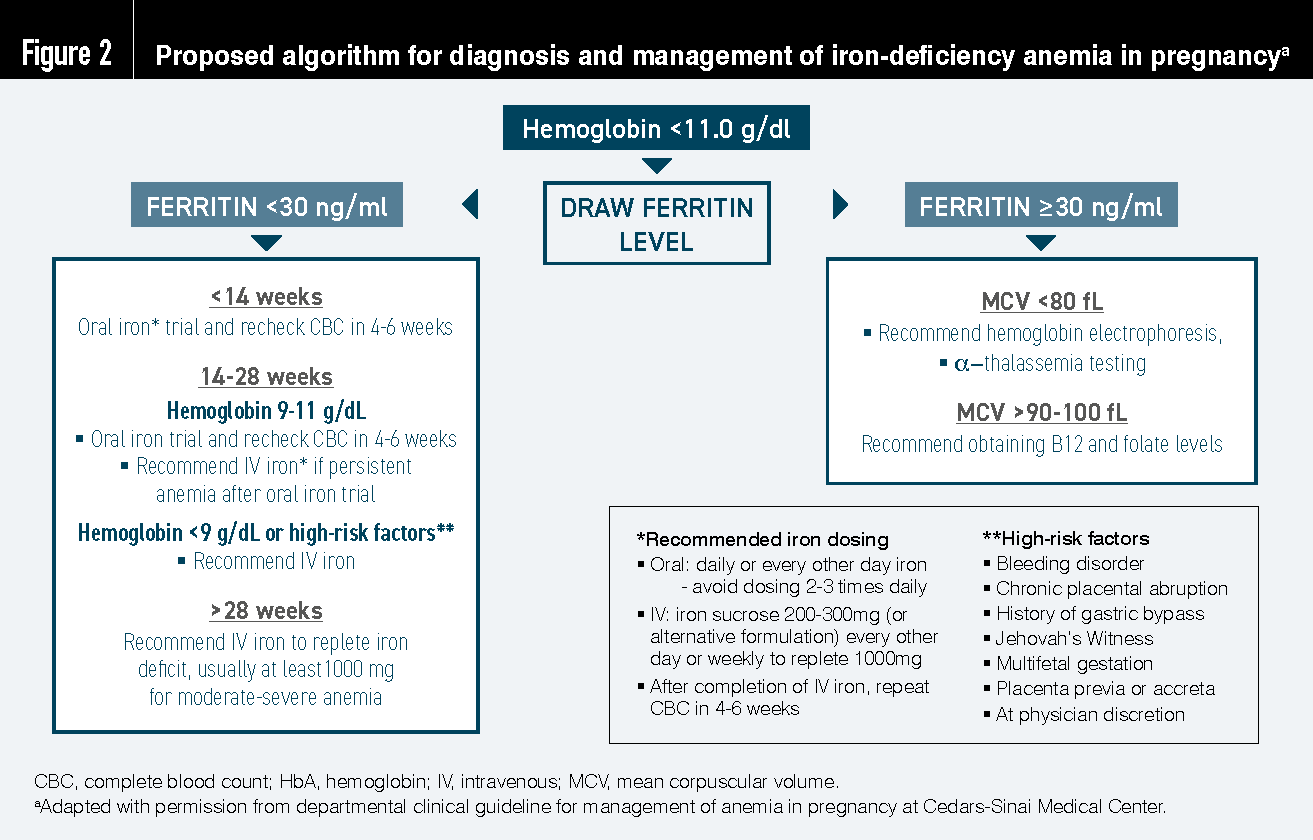
Exact Hemoglobin and Ferritin Thresholds That Trigger IV Iron Treatment
Your healthcare provider relies on specific laboratory benchmarks to determine when oral therapy has failed and intravenous iron becomes medically necessary. These thresholds account for normal pregnancy-related blood dilution while identifying true iron deficiency that requires aggressive intervention.
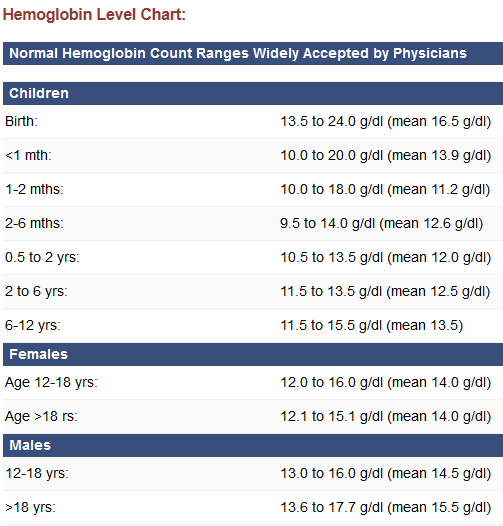
Hemoglobin levels requiring action:
– First trimester: Below 11.0 g/dL
– Second trimester: Below 10.5 g/dL
– Third trimester: Below 11.0 g/dL
Ferritin levels indicating depleted stores:
– Below 30 ng/mL signals depleted iron reserves
– Below 15 ng/mL confirms severe depletion requiring urgent action
These values aren’t absolute—they must be interpreted within your clinical context. Ferritin acts as an acute-phase reactant, meaning inflammation from infections or autoimmune conditions can artificially elevate levels even when true iron deficiency exists. In these cases, your provider will order additional tests including:
- Transferrin saturation (below 20% indicates deficiency)
- Soluble transferrin receptor (elevated in true deficiency)
- Complete blood count with red cell indices
When your hemoglobin falls below 8 g/dL or your ferritin remains below 15 ng/mL despite two weeks of maximum tolerated oral therapy, intravenous iron infusion becomes the standard of care according to current guidelines.
Why Oral Iron Fails for 30-70% of Pregnant Women
Oral iron remains first-line treatment for mild deficiency, but significant limitations make it ineffective for many expectant mothers. Understanding these barriers helps explain why your provider might recommend IV therapy despite your best efforts with pills.
Common reasons oral therapy fails:
- Gastrointestinal intolerance: Constipation affects 50-60% of users, while nausea impacts 30-40%, often worsening morning sickness
- Poor absorption: Only 10-20% of oral iron gets absorbed, with dairy, calcium supplements, and tea reducing uptake further
- Timing conflicts: Taking iron on an empty stomach maximizes absorption but frequently triggers severe nausea
- Malabsorption conditions: Celiac disease, IBD, or gastric bypass surgery can reduce absorption to near zero
Critical timing issues:
– Oral iron requires 2-3 weeks to show hemoglobin improvement
– Full correction takes 8+ weeks—time you may not have in third-trimester diagnoses
– Late-pregnancy iron deficiency leaves insufficient window for oral therapy to work before delivery
When you experience persistent side effects despite trying different formulations (ferrous sulfate, gluconate, or fumarate) or cannot maintain consistent dosing due to gastrointestinal distress, IV iron becomes the clinically appropriate next step.
Specific Clinical Scenarios Requiring IV Iron Infusion
Your provider will consider intravenous iron when one or more of these evidence-based criteria apply to your situation:
Severe Gastrointestinal Intolerance Despite Optimization Attempts
If you’ve experienced persistent nausea, constipation, or abdominal pain with two different oral iron formulations—even when taking reduced doses or using extended-release versions—IV therapy becomes medically indicated. This applies particularly when side effects interfere with your nutrition, hydration, or quality of life.
Third-Trimester Diagnosis with Insufficient Time for Oral Therapy
When iron deficiency is diagnosed after 28 weeks gestation, the 8-12 week timeline needed for oral iron to correct anemia becomes clinically impractical. IV iron delivers therapeutic iron directly into your bloodstream, producing measurable hemoglobin improvement within 7-10 days—critical when delivery approaches.
Hemoglobin Below 8 g/dL Requiring Rapid Correction
At this severity level, maternal oxygen delivery becomes compromised, potentially affecting fetal growth and well-being. While blood transfusion remains necessary for hemoglobin below 7 g/dL, IV iron provides faster correction than oral therapy for levels between 7-8 g/dL, often preventing the need for transfusion.
Documented Malabsorption Conditions
Women with celiac disease, inflammatory bowel disease, or prior gastric bypass surgery typically absorb less than 5% of oral iron. For these patients, IV iron isn’t just an alternative—it’s the only effective treatment pathway.
Safety-First Administration Protocols for Pregnancy
Modern IV iron formulations have dramatically improved safety profiles, but specific protocols ensure maximum protection for you and your baby:
Optimal Timing by Trimester
- Second trimester (weeks 14-27): Preferred window when organogenesis is complete but before peak hemodilution
- Third trimester: Requires careful risk-benefit analysis but often necessary for late diagnoses
- First trimester: Generally avoided unless severe anemia threatens maternal health
Formulation-Specific Protocols
Iron sucrose:
– Dose: 200mg per session
– Sessions: 2-3 weekly infusions
– Infusion time: 15-30 minutes per dose
– Best for: Women with allergy concerns or requiring conservative dosing
Ferric carboxymaltose:
– Dose: 1000-1500mg in single session
– Infusion time: 15 minutes for 1000mg dose
– Best for: Third-trimester cases needing rapid correction
– Critical safety note: Requires weight-based dosing calculation (max 15mg/kg)
Essential Pre-Infusion Screening
Your provider must verify:
– No active infections or inflammatory conditions
– Absence of iron dextran allergy (cross-reactivity risk)
– Normal renal function (creatinine clearance >30 mL/min)
– Current hemoglobin and ferritin levels
What to Expect During and After Your Iron Infusion
Understanding the step-by-step process reduces anxiety and helps you recognize normal versus concerning reactions:
During the Infusion
- First 15 minutes: Infusion runs slowly (1mL/min) while staff monitor for acute reactions
- Common transient effects: Metallic taste (30% of patients), mild headache (20%), flushing (15%)
- Rare but serious signs requiring immediate reporting: Chest tightness, throat swelling, rash, or difficulty breathing
Post-Infusion Monitoring
- Observation period: Minimum 30 minutes after completion
- Delayed reactions: Muscle aches or mild fever may occur 1-2 days post-infusion (self-limiting)
- Paradoxical anemia: Temporary hemoglobin drop 24-48 hours post-infusion due to plasma volume expansion (resolves spontaneously)
Follow-Up Testing Schedule
- Hemoglobin check: 7-10 days post-infusion to assess initial response
- Ferritin recheck: 2-4 weeks after completion to confirm adequate repletion
- Full correction: Typically achieved within 3-4 weeks of treatment
How IV Iron Directly Benefits Your Baby’s Development
Correcting maternal anemia through IV infusion provides crucial advantages for fetal outcomes:
- Third-trimester iron transfer: Your baby accumulates 70% of total iron stores during weeks 28-40
- Neurodevelopmental protection: Adequate iron supports myelination and neurotransmitter synthesis
- Birth weight optimization: Severe maternal anemia correlates with 30% increased risk of low birth weight
Studies show infants born to mothers who received timely IV iron therapy demonstrate:
– Higher cord blood ferritin levels (critical for first 6 months)
– Better Apgar scores at 5 minutes
– Reduced NICU admission rates for anemia-related complications
Postpartum Iron Management After IV Infusion
Your iron needs remain elevated after delivery due to blood loss and breastfeeding demands:
- Immediate postpartum: Expect additional blood loss (500mL vaginal, 1000mL C-section) depleting reserves further
- Breastfeeding requirements: 0.5mg iron daily transferred to breast milk
- Essential follow-up: Hemoglobin and ferritin checks at 4-6 weeks postpartum
Women who received IV iron during pregnancy typically require:
– 30-60mg elemental iron daily while breastfeeding
– Dietary emphasis on heme iron sources (meat, fish, poultry)
– Vitamin C-rich foods to enhance non-heme iron absorption
Key Decision Points for Patients Considering IV Iron
When discussing this treatment with your provider, focus on these critical questions:
- “What specific lab values indicate I need IV rather than oral iron?”
- “Which formulation do you recommend and why, based on my specific situation?”
- “What’s the exact timing plan for my infusion relative to my due date?”
- “What emergency protocols are in place if I react during the infusion?”
Remember that choosing IV iron isn’t a failure of oral therapy—it’s a medically appropriate escalation when your unique physiology or pregnancy timeline requires more aggressive intervention. Current guidelines support IV iron as a safe, effective option when administered according to evidence-based protocols, offering both you and your baby the iron resources needed for a healthy outcome.



