Parents of children with ADHD know the daily struggle with focus, impulse control, and hyperactivity that impacts school performance, family dynamics, and self-esteem. While stimulant medications remain standard treatment, emerging research points to an unexpected factor influencing symptom severity: iron deficiency. Clinical trials demonstrate that children with ADHD and low iron stores often experience meaningful symptom improvement with iron supplementation. Understanding the iron-ADHD connection offers parents and healthcare providers an additional strategy—particularly for children who don’t fully respond to standard treatments or show documented iron deficiency.
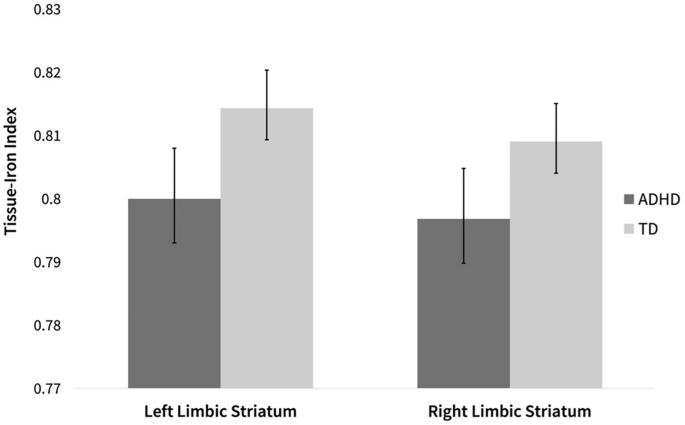
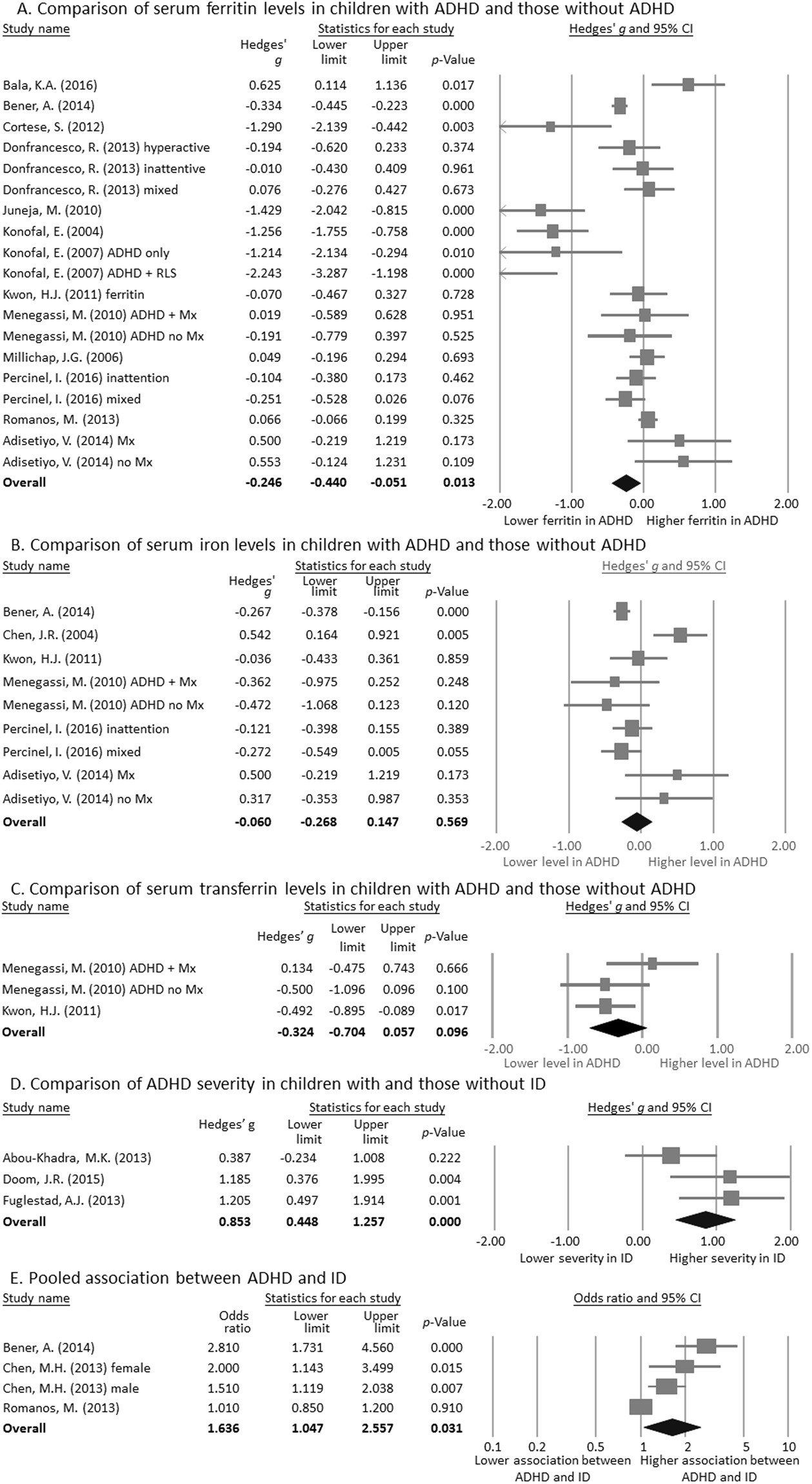
Iron’s role extends far beyond preventing anemia—it’s a critical cofactor for enzymes involved in dopamine synthesis, the neurotransmitter central to attention regulation. Children with ADHD consistently show lower serum ferritin levels (the primary marker of iron stores) compared to neurotypical peers, with deficiency severity correlating directly to symptom severity. Brain imaging studies confirm lower iron levels in the thalami of children with ADHD, revealing a biological basis for why iron supplementation may enhance traditional ADHD management strategies when combined appropriately.
Why Low Ferritin Levels Worsen ADHD Symptoms in Children
Children with ADHD show dramatically higher rates of iron deficiency than their peers, with research revealing 84% of ADHD children have serum ferritin below 30 ng/mL compared to just 18% of controls. This iron deficiency directly impacts brain function through multiple mechanisms: it reduces tyrosine hydroxylase activity (the rate-limiting enzyme in dopamine production), impairs myelin formation, and disrupts norepinephrine and serotonin metabolism. Without adequate iron, dopamine synthesis falters, directly affecting attention regulation and behavioral control pathways.
Children with low iron stores—even without anemia—experience decreased attention capacity, impaired motor function, memory difficulties, and emotional instability. Animal models demonstrate decreased dopamine receptor density and impaired monoamine transporter function during iron deficiency, providing the biological explanation for why iron status significantly influences ADHD symptom presentation. The developing brain appears particularly vulnerable to these neurochemical changes, making iron assessment crucial in pediatric ADHD management.
Konofal Study: How 80 mg Iron Daily Reduces ADHD Rating Scale Scores
The landmark Konofal study provided the first rigorous evidence that iron supplementation improves ADHD symptoms in iron-deficient children. This double-blind, placebo-controlled trial enrolled 23 nonanemic children aged 5-8 with ADHD and serum ferritin below 30 ng/mL. Participants received either 80 mg elemental iron daily as ferrous sulfate or placebo for 12 weeks, with results showing a statistically significant 11-point decrease in ADHD Rating Scale scores in the iron group (P<0.008) compared to minimal change in placebo.
Secondary measures confirmed these findings—the Clinical Global Impression-Severity scale showed significant symptom improvement in the iron group while placebo remained stable. Notably, restless legs syndrome symptoms (common in ADHD and linked to dopamine dysfunction) also improved with iron supplementation. This study established that iron repletion alone can meaningfully reduce core ADHD symptoms in children with documented deficiency, offering a safe, low-cost intervention option.
Ferrous Sulfate With Methylphenidate: 12-Week Protocol for Maximum Benefit
Research demonstrates iron supplementation works best as an adjunct to standard ADHD medications. The Tohidi study evaluated 50 children already taking methylphenidate who also had low ferritin (<30 ng/mL). Half received 80 mg elemental iron daily alongside their existing medication, while the other half received placebo. After 12 weeks, the iron group showed significant improvements in conduct problems (P=0.003) and psychosomatic symptoms that weren’t present in the methylphenidate-only group.
Key findings from combination therapy studies:
– Serum ferritin increased from 21 ng/mL to 47 ng/mL in successfully treated children
– Benefits emerged gradually, with significant improvements appearing primarily during weeks 6-12
– Both attention deficit and hyperactive/impulsive subscale scores improved significantly
– Total symptom scores decreased more markedly with combination therapy (P=0.002)
This evidence supports iron supplementation as a complementary treatment—not a replacement—for standard ADHD therapies, particularly for children with incomplete response to stimulants alone.
Who Needs Ferritin Testing: Identifying Iron-Deficient ADHD Children
Not all children with ADHD require iron supplementation—only those with documented deficiency. Optimal candidates have:
– Confirmed ADHD diagnosis
– Serum ferritin levels below 30 ng/mL
– No evidence of anemia (normal hemoglobin)
Certain symptoms may signal underlying iron deficiency in ADHD children:
– Restless legs syndrome (irresistible urge to move legs, worse at night)
– Unexplained fatigue or decreased activity tolerance
– Pale skin or brittle nails
– Poor appetite despite adequate growth
Baseline testing should include serum ferritin as the primary indicator of iron stores, plus complete blood count to rule out anemia. Children with ferritin levels above 30 ng/mL are unlikely to benefit from supplementation and may risk iron overload with unnecessary treatment.
Managing Ferrous Sulfate Side Effects Without Reducing Effectiveness
:max_bytes(150000):strip_icc()/do-iron-supplements-for-anemia-cause-upset-stomach-3522504-01-a8806fc982ab45998d75000e183bc406.png)
Iron supplementation demonstrates excellent tolerability in clinical trials, with most side effects being mild and transient:
– Constipation affects approximately 9% of children
– Intermittent abdominal pain occurs in about 13.6% of cases
– Most gastrointestinal symptoms resolve within weeks despite continued treatment
Proven strategies to minimize side effects:
– Start with half-dose for first week, then increase to full dose
– Take with small amount of food if stomach upset occurs (reduces but doesn’t eliminate absorption)
– Avoid calcium-rich foods and antacids within 2 hours of dosing
– Consider alternative formulations like ferrous gluconate if sulfate causes persistent issues
Notably, 18.1% of children in iron studies reported increased appetite—a potential benefit since iron deficiency often suppresses appetite. Only two children discontinued treatment due to side effects in the largest trial, compared to three in the placebo group, confirming iron’s favorable safety profile.
Maximizing Iron Absorption for Better ADHD Symptom Control
How you administer iron significantly impacts its effectiveness for ADHD symptom management. Research shows these evidence-based strategies maximize absorption:
Optimal timing:
– Administer in morning to align with natural iron metabolism cycles
– Space doses at least 2 hours from calcium-containing foods or supplements
– Separate from antacids or proton pump inhibitors by 4+ hours
Absorption boosters:
– Pair with vitamin C-rich foods (orange juice, strawberries, bell peppers)
– Avoid tea, coffee, or dairy within 2 hours of dosing
– Consider liquid formulations if swallowing pills causes issues
Dosing protocol:
– 80 mg elemental iron daily as ferrous sulfate (300 mg capsule)
– Weight-based alternative: 5 mg/kg body weight for children
– Continue for minimum 12 weeks to assess full therapeutic effect
Tracking Your Child’s Response to Iron Supplementation
Effective monitoring ensures you recognize improvements and adjust treatment appropriately. Implement this tracking system:
Symptom assessment:
– Use validated rating scales like Conners’ Parent Rating Scale weekly
– Focus on specific changes in conduct problems, learning difficulties, and psychosomatic symptoms
– Note improvements in restless legs syndrome if present
Laboratory monitoring:
– Repeat ferritin test after 8-12 weeks to confirm repletion
– Target ferritin level above 30 ng/mL for therapeutic effect
– Check complete blood count to monitor for developing anemia
Timeline for expected changes:
– Weeks 1-4: Possible gastrointestinal adjustment period
– Weeks 4-8: Early improvements in conduct and learning problems
– Weeks 8-12: Significant reductions in overall symptom severity
Parents should maintain detailed symptom logs and share them with their child’s healthcare provider at follow-up appointments to guide treatment decisions.
Iron Supplement Protocol for ADHD: What Parents Need to Know
Implementing iron supplementation requires careful planning and realistic expectations. Start by discussing testing with your child’s pediatrician—serum ferritin testing is simple and covered by most insurance plans. If levels fall below 30 ng/mL without anemia, supplementation may be appropriate alongside existing treatments.
Consistency is critical—administer iron at the same time daily and track symptoms in a simple journal. Understand that benefits develop gradually over 2-3 months, not immediately like stimulant medications. Continue all established ADHD interventions while adding iron, rather than replacing them.
The cost advantage makes iron supplementation accessible—generic ferrous sulfate costs just a few dollars monthly. This affordability provides hope for families seeking additional support, particularly when standard treatments alone don’t provide complete symptom control.
Key Takeaways: Iron Supplementation as Adjunct ADHD Treatment
Iron supplementation offers a safe, inexpensive strategy to enhance ADHD management in iron-deficient children. Clinical evidence confirms that ferrous sulfate providing 80 mg elemental iron daily for 12 weeks improves conduct problems, learning difficulties, and overall symptom severity in children with ferritin below 30 ng/mL. The greatest benefits occur when iron supplementation complements standard methylphenidate therapy rather than replacing it.
Parents should consider ferritin testing for children with ADHD who show incomplete response to standard treatments or exhibit symptoms suggesting iron deficiency. With proper administration and monitoring, iron supplementation represents a valuable addition to comprehensive ADHD management—one that addresses the underlying neurobiology of attention regulation through dopamine pathway support. While not a standalone solution, this approach offers meaningful symptom improvement for a significant subset of children with ADHD and documented iron deficiency.