
If you’re managing chronic kidney disease, understanding the connection between low iron and kidney disease is essential for your overall health and quality of life. Iron deficiency anemia affects up to 90% of dialysis patients and significantly impacts those with earlier-stage kidney disease too. When kidney function declines, your body’s ability to maintain healthy iron levels becomes compromised through multiple mechanisms—reduced hormone production, chronic inflammation, and blood losses during dialysis. This article explains exactly why low iron occurs with kidney disease, how to recognize it, and what treatment options work best for your specific situation.
7 Mechanisms Linking Kidney Damage to Iron Depletion

Kidney disease triggers iron deficiency through several physiological pathways that most patients never learn about during routine appointments. Understanding these mechanisms helps explain why simply taking iron supplements might not solve your problem if you have kidney disease.
How Damaged Kidneys Disrupt Erythropoietin Production
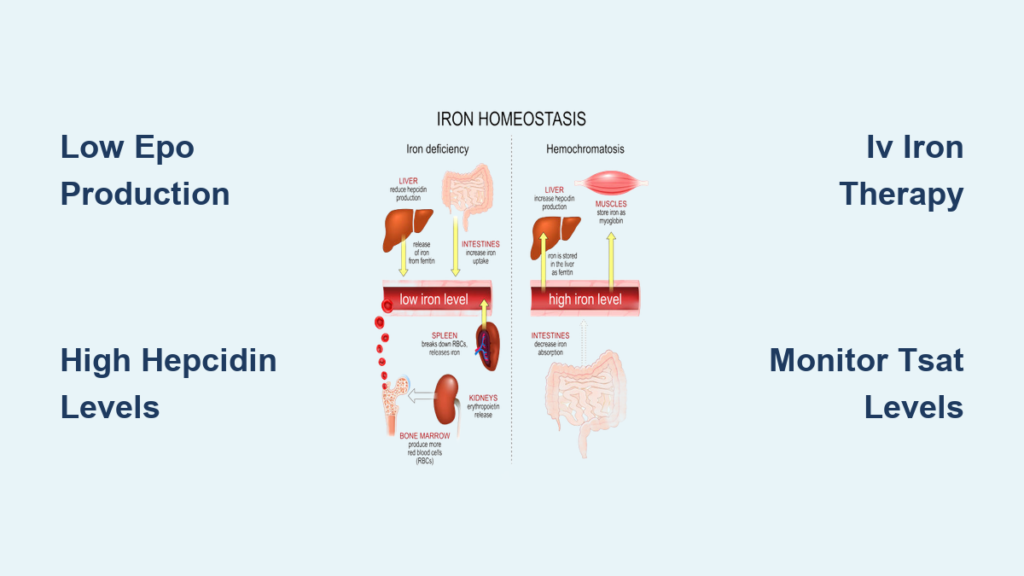
Your kidneys produce erythropoietin (EPO), the hormone that signals your bone marrow to make red blood cells. As kidney function declines, EPO production drops significantly—sometimes to just 10-20% of normal levels. Without sufficient EPO, your body can’t effectively utilize available iron for red blood cell production, creating anemia even when iron stores appear adequate.
The connection between low iron and kidney disease intensifies when inflammation elevates hepcidin, the master iron-regulating hormone. Damaged kidneys clear less hepcidin, causing levels to rise and effectively “lock” iron in storage sites. This prevents iron from reaching your bone marrow regardless of how much you consume through diet or supplements.
Dialysis-Specific Iron Loss Factors
If you’re on hemodialysis, you face additional iron depletion mechanisms that most patients don’t realize:
- Blood loss during each session: Up to 2-3 grams of iron lost per year through the dialysis circuit
- Frequent blood draws: Multiple weekly lab tests gradually deplete your iron reserves
- Impaired iron absorption: Chronic inflammation reduces your gut’s ability to absorb oral iron
- Medication interference: Phosphate binders commonly prescribed for kidney disease bind to iron in your digestive tract
These factors combine to create a perfect storm where maintaining adequate iron becomes increasingly difficult as kidney function declines.
Absolute vs. Functional Iron Deficiency: How to Identify Your Type

Not all low iron and kidney disease cases represent the same problem. Understanding which type you have determines the most effective treatment approach and prevents wasted time on ineffective therapies.
Absolute Iron Deficiency: When Your Body Runs Out of Iron
Absolute iron deficiency occurs when your total iron stores become severely depleted. In kidney disease patients, this typically develops through:
- Chronic blood loss (from dialysis or gastrointestinal issues)
- Inadequate dietary intake
- Poor absorption due to medications
Key diagnostic markers:
– Serum ferritin < 100 ng/mL (predialysis) or < 200 ng/mL (hemodialysis)
– Transferrin saturation ≤ 20%
– Microcytic (small), hypochromic (pale) red blood cells
If you have absolute iron deficiency, your body literally lacks the raw materials needed to make hemoglobin, regardless of how much EPO your kidneys produce.
Functional Iron Deficiency: Iron Locked Away Despite Adequate Stores
This more complex condition affects many kidney disease patients and often causes confusion when lab results seem contradictory. In functional iron deficiency, your body has sufficient iron stores but can’t access them due to:
- Elevated hepcidin levels from chronic inflammation
- Reduced kidney clearance of hepcidin
- Impaired iron transport mechanisms
Key diagnostic markers:
– Normal or high ferritin levels (often > 500 ng/mL)
– Transferrin saturation ≤ 20%
– Normal or large red blood cells
You might receive EPO-stimulating medications but see little improvement because your bone marrow can’t access the iron needed to produce red blood cells.
10 Warning Signs Your Kidney Disease Has Triggered Iron Deficiency
Recognizing these symptoms early can prevent complications and improve your quality of life. Many kidney disease patients mistakenly attribute these to their kidney condition alone.
Physical Symptoms You Shouldn’t Ignore
- Persistent fatigue that doesn’t improve with rest
- Unusual shortness of breath during normal activities
- Pale skin, especially noticeable in your lower eyelids
- Rapid heartbeat or heart palpitations
- Dizziness when standing up quickly
- Brittle nails and hair loss
- Cold hands and feet even in warm environments
- Difficulty concentrating or “brain fog”
- Worsening of existing heart conditions
- Unusual cravings for ice (a condition called pagophagia)
If you’re on EPO-stimulating medications but notice decreasing effectiveness, this often signals developing iron deficiency that needs immediate attention.
Decoding Your Iron Tests: Why Standard Guidelines Don’t Apply to Kidney Patients
Standard iron deficiency diagnosis criteria don’t work for kidney disease patients because inflammation alters key markers. Your healthcare team must interpret results differently.
Critical Lab Values and Kidney-Specific Thresholds
Transferrin saturation (TSAT):
– Normal range: 20-50%
– Kidney disease target: ≥ 30% (below 20% indicates deficiency)
– Action step: Request this test at every 3-month checkup if you have CKD
Serum ferritin:
– Normal range: 15-150 ng/mL
– Kidney disease thresholds:
– Predialysis: < 100 ng/mL indicates absolute deficiency
– Hemodialysis: < 200 ng/mL indicates absolute deficiency
– Warning: Inflammation elevates ferritin independently of iron stores
Common diagnostic mistake: Assuming normal ferritin means adequate iron when TSAT is low—this indicates functional iron deficiency requiring different treatment.
IV vs. Oral Iron: Which Works Best for Your Stage of Kidney Disease
Choosing the right iron therapy depends on your kidney disease stage, dialysis status, and specific iron deficiency type.
Intravenous Iron: The Gold Standard for Dialysis Patients
For hemodialysis patients, IV iron works significantly better than oral supplements because:
- Bypasses impaired gut absorption
- Provides immediate iron availability
- Requires fewer doses (often administered during dialysis sessions)
- Reduces needed EPO medication doses by 25-30%
Most effective IV iron formulations:
– Ferric carboxymaltose (single higher doses)
– Iron sucrose (multiple smaller doses)
– Ferumoxytol (for patients with residual kidney function)
Pro tip: Ask about “iron repletion” protocols that rapidly restore stores before transitioning to maintenance doses.
Oral Iron: When It Might Work for Earlier-Stage Kidney Disease
If you have CKD stages 3-4 without dialysis, oral iron may be appropriate if:
- You have absolute iron deficiency
- Your TSAT is very low (<15%)
- You don’t have significant inflammation
Maximize absorption with these strategies:
1. Take iron on empty stomach (1 hour before meals)
2. Wait 2 hours after taking phosphate binders or calcium supplements
3. Pair with vitamin C (orange juice) to enhance absorption
4. Avoid coffee/tea within 2 hours of dosing
Common mistake: Stopping oral iron due to side effects—ask about newer formulations like iron protein succinylate that cause less constipation and nausea.
Preventing Heart Damage from Low Iron in Advanced Kidney Disease
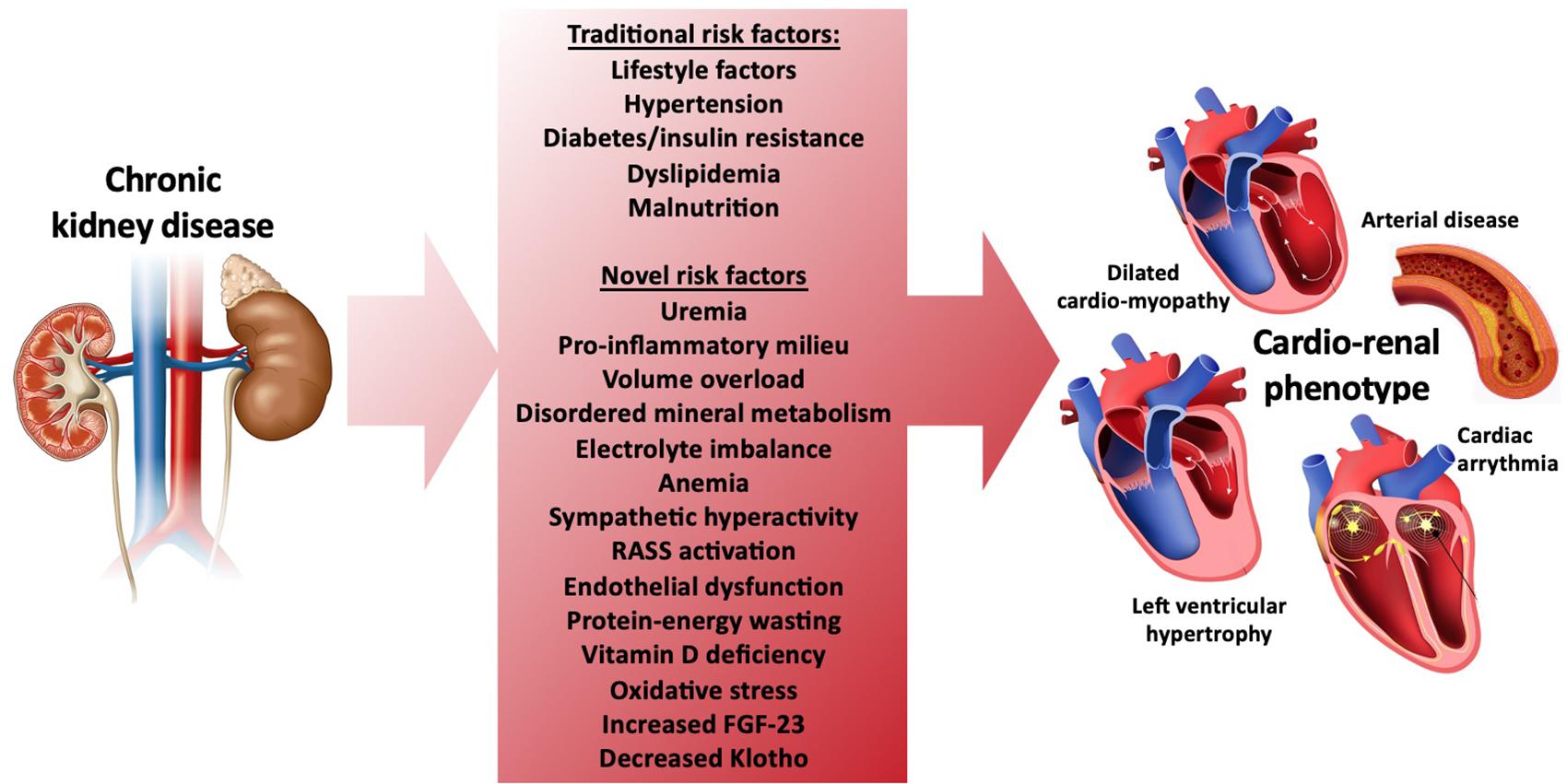
Untreated low iron and kidney disease significantly increases your risk of cardiovascular complications—the leading cause of death in CKD patients.
How Iron Deficiency Strains Your Heart
When hemoglobin drops below 10 g/dL:
– Your heart pumps 20-30% harder to deliver oxygen
– Cardiac output increases by up to 50%
– Left ventricular hypertrophy develops in 70% of untreated patients
Critical action steps:
– Maintain hemoglobin between 10-11 g/dL (higher targets increase risks)
– Monitor iron status quarterly if on dialysis
– Report new or worsening shortness of breath immediately
Research shows correcting iron deficiency reduces hospitalizations for heart failure by 28% in dialysis patients—making proper iron management potentially lifesaving.
Daily Strategies to Maintain Iron Balance with Chronic Kidney Disease
Managing low iron with kidney disease requires an ongoing partnership between you and your healthcare team. These practical approaches make a significant difference.
Your Action Plan for Iron Management
- Track symptoms: Note fatigue levels daily using a 1-10 scale
- Coordinate timing: Schedule iron doses away from phosphate binders
- Dietary support: Include moderate heme iron sources (chicken, fish) within your kidney diet
- Communication: Ask for your TSAT and ferritin results at every visit
- Advocate: Request iron studies if EPO medications become less effective
When to seek immediate help:
– Unexplained chest pain
– Severe shortness of breath at rest
– Heart rate consistently over 100 bpm
– Sudden worsening of fatigue
Remember that successfully managing low iron and kidney disease isn’t just about correcting lab values—it’s about preserving your energy, protecting your heart, and maintaining the quality of life you deserve. With proper monitoring and treatment tailored to your specific needs, you can effectively manage this common but treatable complication of kidney disease.



