You’ve tried everything—thyroid medication, iron supplements, more sleep—but that crushing fatigue, stubborn weight gain, and brain fog persist. What if two seemingly unrelated conditions are working against you simultaneously? Research confirms a powerful bidirectional relationship between low iron and underactive thyroid function, where insufficient iron stores directly impair thyroid hormone production while thyroid dysfunction simultaneously disrupts how your body processes iron. This hidden connection explains why standard treatments often fail to resolve persistent symptoms.
If you’ve been diagnosed with hypothyroidism but still feel exhausted despite medication, or if iron supplements haven’t resolved your fatigue, you’re likely caught in this vicious cycle. The good news: understanding this relationship provides the key to finally breaking free from unexplained symptoms that have plagued you for months or years.
How Iron Deficiency Sabotages Your Thyroid Hormone Production
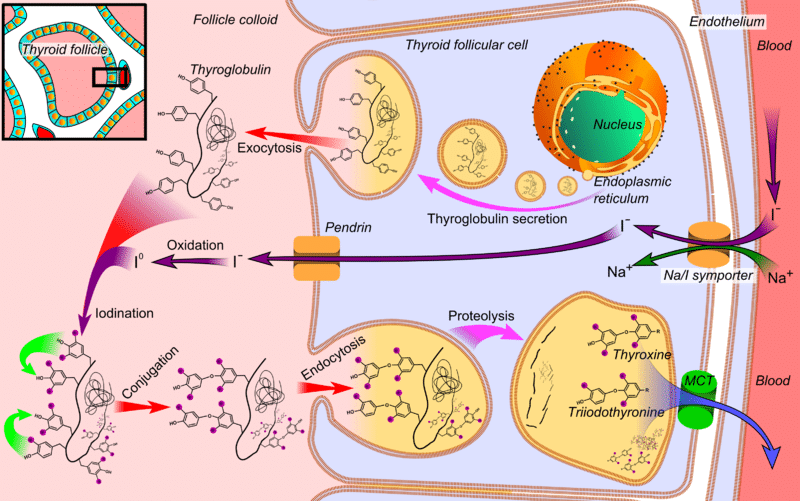
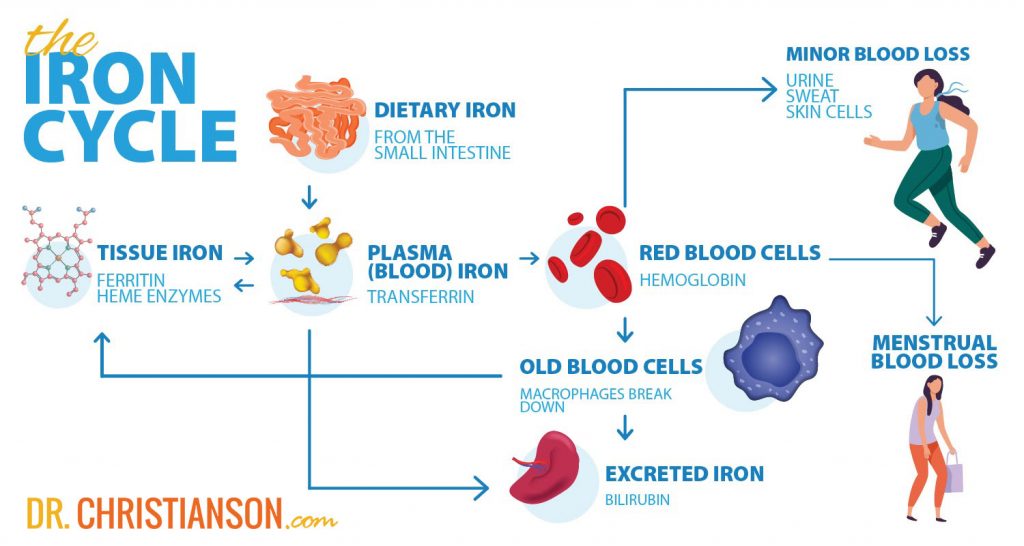
Iron isn’t just for blood—it’s essential for proper thyroid function at the most fundamental level. The thyroid peroxidase enzyme (TPO), which requires iron as its central component, catalyzes the critical reactions needed to produce thyroid hormones. Without adequate iron, TPO can’t efficiently convert iodide to iodine or attach it to tyrosine residues in thyroglobulin, directly limiting your thyroid’s ability to make sufficient thyroxine (T4) and triiodothyronine (T3).
Why Thyroid Peroxidase Needs Iron to Function
TPO is a hemoprotein that depends entirely on iron within its prosthetic groups to function as an oxidizing agent. When your iron stores run low, this enzyme becomes compromised, disrupting the very first steps of thyroid hormone synthesis. Studies show iron-deficient individuals demonstrate significantly lower free thyroxine (FT4) concentrations—averaging 1.18 pmol/L lower—compared to iron-replete controls. This explains why your thyroid medication might seem ineffective: your body literally can’t produce enough active hormone to convert, regardless of how well your medication is absorbed.
The Missing Link: Iron’s Role in T4 to T3 Conversion
Even if your thyroid produces some T4, iron deficiency sabotages your body’s ability to convert it to the active T3 form. Iron participates in the activity of thyroxine deiodinase enzymes responsible for this conversion. Without adequate iron, this process becomes inefficient, leaving you with “normal” TSH levels but functional hypothyroidism—where your cells starve for active thyroid hormone despite seemingly adequate production. This is why you might experience classic hypothyroid symptoms even when blood tests appear borderline.
Why Hypothyroidism Worsens Iron Deficiency
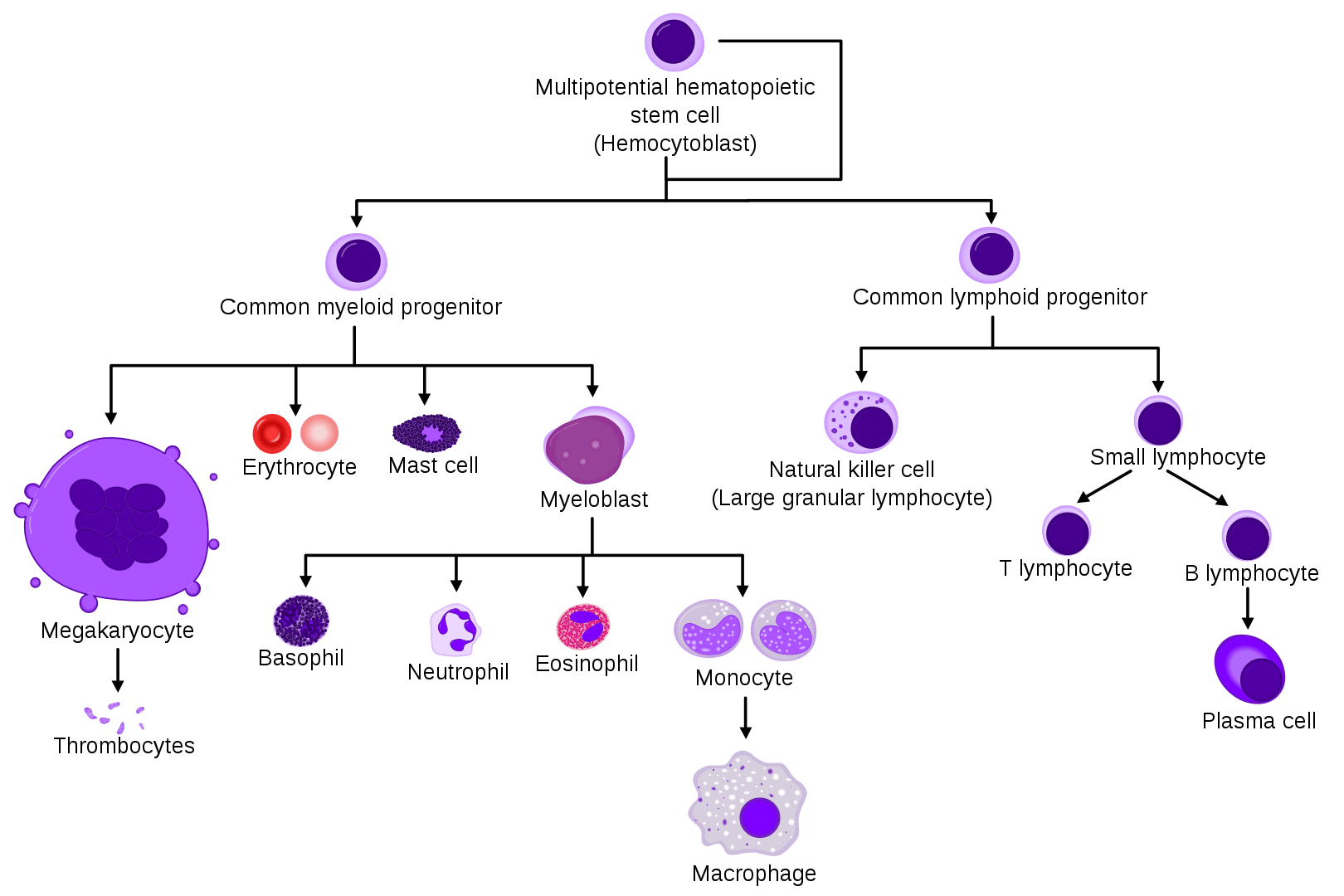
Thyroid dysfunction doesn’t just suffer from low iron—it actively makes iron deficiency worse through multiple mechanisms. Thyroid hormones directly stimulate red blood cell production by binding to thyroid receptor alpha (TRα) receptors on erythrocyte precursors. When your thyroid underperforms, this stimulation diminishes significantly, reducing your body’s ability to utilize iron for hemoglobin synthesis.
How Thyroid Hormones Control Red Blood Cell Production
Your thyroid hormones are primary regulators of erythropoiesis—the process of red blood cell formation. In hypothyroid states, the proliferation of erythrocyte precursors slows dramatically, creating a situation where even adequate iron intake can’t be properly utilized. This explains why simply taking iron supplements often fails to resolve anemia in people with untreated hypothyroidism—their bodies literally can’t process the iron effectively without sufficient thyroid hormone.
The Erythropoietin Connection in Thyroid Dysfunction
Hypothyroidism also reduces your kidneys’ production of erythropoietin, the hormone that signals your bone marrow to produce more red blood cells. With lower erythropoietin levels, your body doesn’t trigger the necessary red blood cell production even when iron is available. This creates a self-perpetuating cycle: low thyroid function reduces erythropoietin, which reduces red blood cell production, which worsens fatigue and other symptoms, making it harder to address either condition effectively.
Recognizing the Dual Deficiency Symptoms
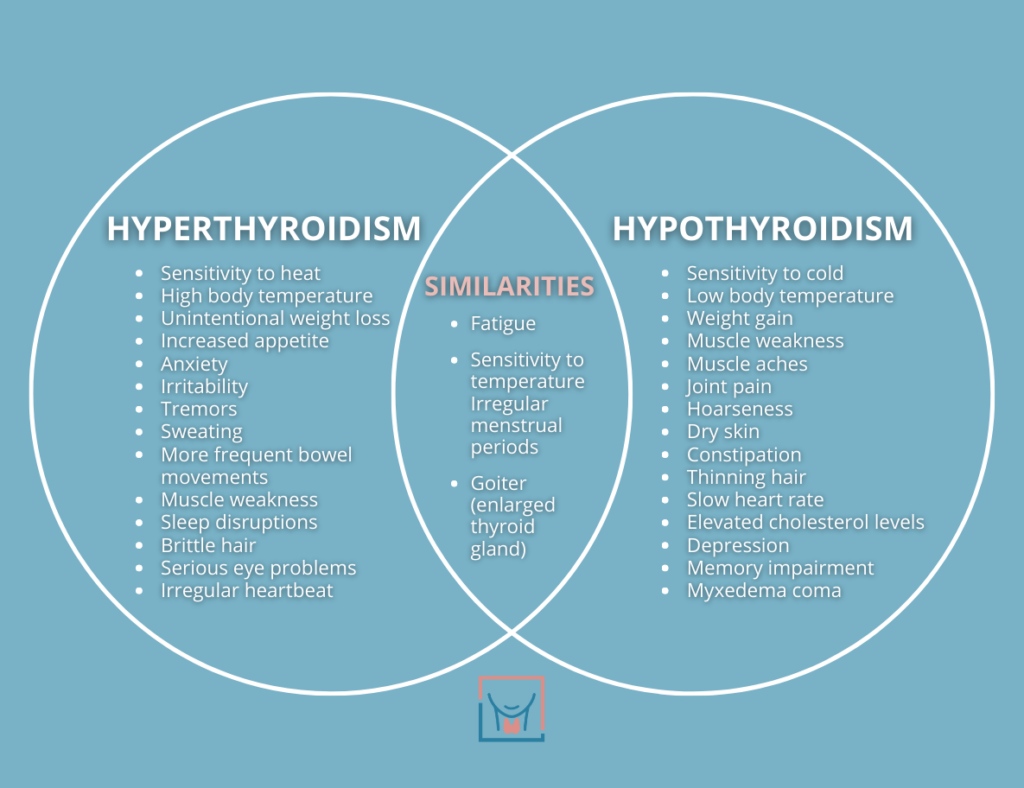
Identifying concurrent low iron and underactive thyroid can be challenging because symptoms overlap significantly. Fatigue—the most common symptom of both conditions—often leads doctors to diagnose only one issue while the other goes undetected. However, certain symptom combinations should raise suspicion of this dual deficiency.
Overlapping Symptoms That Confuse Diagnosis
Both conditions cause fatigue, pale skin, hair loss, cold intolerance, and brain fog. But when you experience unusual cravings for ice or dirt alongside hypothyroid symptoms like constipation and weight gain despite no dietary changes, this strongly suggests concurrent iron deficiency. Similarly, if you have restless leg syndrome combined with dry skin and menstrual irregularities, you’re likely dealing with both issues simultaneously.
The Specific Warning Signs of Combined Iron and Thyroid Issues
Watch for these red flags indicating both conditions:
– Persistent fatigue that doesn’t improve with thyroid medication alone
– Brittle nails that continue breaking despite iron supplementation
– Shortness of breath during ordinary activities combined with cold intolerance
– Heavy menstrual periods that don’t respond to standard treatments
These symptom combinations often indicate that treating only one condition won’t resolve your issues—you need to address both simultaneously.
High-Risk Groups Most Vulnerable to This Double Deficit
Certain populations face dramatically increased risk for developing both low iron and underactive thyroid simultaneously. Understanding your risk level helps determine whether comprehensive testing is warranted.
Why Pregnant Women Face Double Trouble with Iron and Thyroid
Pregnant women represent the most vulnerable population due to dramatically increased iron requirements from expanded blood volume and fetal demands. Research shows iron-deficient pregnant women exhibit significantly higher TSH and lower FT4 than iron-replete women. The stakes are particularly high because maternal thyroid hormones are essential for fetal brain development during the first trimester—before the baby’s own thyroid functions. If left unaddressed, this dual deficiency increases risks for gestational diabetes, preeclampsia, and neurological deficits in offspring.
Women of Childbearing Age: The Silent Struggle with Iron and Thyroid
Monthly blood loss through menstruation creates ongoing iron demands that many women struggle to meet. Studies confirm non-pregnant women with iron deficiency demonstrate significantly lower FT4 and FT3 levels—averaging 0.72 pmol/L lower for FT4—compared to iron-replete women. These same women also show double the rate of thyroid autoantibodies (8.37% vs. 3.87%), suggesting iron deficiency may accelerate autoimmune thyroid damage. If you’re a woman experiencing unexplained fatigue, comprehensive testing for both iron and thyroid status is essential.
Diagnostic Tests That Reveal the Hidden Connection
Proper diagnosis requires going beyond basic screening. Serum ferritin is the most important indicator of iron stores, but many doctors stop at hemoglobin levels, missing early iron deficiency that still affects thyroid function.
Why Ferritin Below 30 ng/dL Should Raise Thyroid Concerns
While many labs consider ferritin above 15 ng/dL as “normal,” research shows ferritin below 30 ng/dL correlates with lower thyroid hormone levels. Some experts recommend targeting ferritin above 50-70 ng/dL for optimal thyroid health, especially if you have thyroid dysfunction. If your ferritin is in the 20-30 ng/dL range and you have hypothyroid symptoms, this may explain why standard treatments aren’t working.
Interpreting Thyroid Panels When Iron Is Low
Relying solely on TSH can be misleading with iron deficiency. The research shows iron-deficient pregnant women actually have lower TSH levels despite having lower FT4 and FT3. For accurate assessment, you need a complete panel including:
– TSH
– Free T4
– Free T3
– Thyroid peroxidase antibodies (TPOAb)
– Ferritin
A pattern of low-normal FT4 with normal TSH in an iron-deficient person should prompt investigation into this bidirectional relationship.
Breaking the Cycle: Effective Treatment Strategies
Addressing both conditions simultaneously produces dramatically better results than treating either one alone. The evidence shows restoring adequate iron stores promotes recovery of normal thyroid function, with serum ferritin normalization correlating with improved thyroid hormone concentrations.
Iron Supplementation Protocols That Restore Thyroid Function
For effective iron repletion:
– Take 65-100 mg of elemental iron daily on an empty stomach with vitamin C
– Avoid calcium, zinc, coffee, and tea within two hours of iron supplements
– Consider intravenous iron if you have gastrointestinal side effects or malabsorption conditions
– Retest ferritin after 3 months to ensure adequate repletion
Studies demonstrate that iron-deficient individuals with subclinical hypothyroidism show significantly better outcomes with combined iron and thyroid treatment compared to either intervention alone.
Optimizing Thyroid Medication When Iron Is Deficient
Continue your thyroid medication as prescribed while addressing iron deficiency. However, be aware that thyroid medication requirements may change once iron stores normalize. Regular monitoring of both iron status and thyroid function during repletion allows for appropriate medication adjustments. Some patients find their required thyroid medication dose decreases after iron repletion as their natural thyroid function improves.
Preventing the Iron-Thyroid Deficiency Cycle
Breaking this cycle requires ongoing attention to both nutritional status and thyroid health. For those who have experienced iron deficiency, annual ferritin testing provides early warning of depleting iron stores before they affect thyroid function.
Dietary Strategies to Support Both Iron and Thyroid Health
Make these dietary patterns permanent lifestyle changes:
– Consume heme iron sources (red meat, poultry, fish) for best absorption
– Pair non-heme iron foods (leafy greens, legumes) with vitamin C-rich foods
– Limit coffee and tea consumption to between meals rather than with meals
– Ensure adequate but not excessive iodine intake through balanced diet
These simple changes maintain iron stores while supporting optimal thyroid function, preventing the recurrence of this debilitating cycle.
If you’ve struggled with persistent fatigue despite treatment for either iron deficiency or hypothyroidism, request comprehensive testing for both conditions. Addressing this hidden connection could finally resolve the symptoms that have undermined your health and quality of life for far too long.